Actively Engaged and the Comprehensive Provider Attribution (CPA)
New York Regional Extension Center (REC) Footprint
- Presentation is also available in Portable Document Format (PDF)
March 2016
Agenda
- Level Set: PPS Patient Engagement Targets will be adjusted
- Agenda:
Actively Engaged Reporting in IPP
Actively Engaged Reporting Requirements
- PPS are required to report updates to their Actively Engaged counts in each quarterly report for each project with an Actively Engaged (AE) commitment
- The quarterly reporting of Actively Engaged counts is cumulative throughout a DSRIP Year (DY), unless specifically noted in the Actively Engaged definition for a project
- Duplicate counts of members are not allowed, unless specifically noted for a project
DY2, Q1 (Medicaid members engaged during DY2, Q1 only) DY2, Q2 (Medicaid members engaged during DY2, Q2 only) DY2, Q2 (AE Count reported on DY2, Q2 Quarterly Report) 500 800 1,300
- PPS must engage a minimum of 80% of the Actively Engaged commitment target for a quarter in order to earn the Achievement Value (AV) for this milestone for that quarter.
- The 80% minimum standard was reduced to 75% for DY1, Q2.
Medicaid Member Registry Requirement
- PPS must be able to substantiate the Actively Engaged counts reported on the quarterly reports through a registry of Medicaid members maintained by the PPS and submitted through IPP to the Independent Assessor.
For each Medicaid member engaged by the PPS and network partners, the registry must include, at a minimum: - The Medicaid Client Identification Number (CIN)
- The Medicaid Managed Care Policy Number
- For Project 2.d.i – a Unique Individual Identifier
- An exception has been made to accommodate data sharing concerns associated with Medicaid members with substance use disorder (SUD) under 42 CFR. PPS are able to submit attestations from the SUD providers to support the Actively Engaged counts in lieu of the CIN data.
Actively Engaged Validation
- Actively Engaged counts will be validated by the Independent Assessor each quarter where the PPS has an Actively Engaged commitment target
- Actively Engaged supporting documentation must be submitted with the initial submission of the quarterly report
- Actively Engaged is not subject to the remediation process, however PPS can submit additional documentation to the Independent Assessor through remediation if the PPS identifies an error with the original submission
- PPS that miss their Actively Engaged commitment targets in Q1 or Q3 may still earn the AV and associated performance payments if the cumulative totals through Q2 and Q4 reach the 80% of commitment target threshold for these quarters.
Double Counting a Medicaid Member
- PPS cannot "double count" a Medicaid member in their Actively Engaged reporting
- The ´double count´ applies when multiple PPS are pursuing the same project and share network partners and is intended to ensure that the same Medicaid member is not counted by multiple PPS under the same project.
| PPS A and PPS B are implementing project 3.a.i and both have Mental Health Provider 1 in their networks. |
| ↓ |
| Mental Health Provider 1 engages 1,000 Medicaid members for project 3.a.i during DY2, Q2. |
| ↓ |
| PPS A and PPS B must split the 1,000 Actively Engaged Medicaid members from Mental Health Provider 1 for project 3.a.i so the total count from this provider across the two PPS does not exceed 1,000 |
Actively Engaged Discount Methodology
Introduction
- Because of the lack of clarity in previously communicated active patient engagement guidance, a discount factor has been applied to relevant projects
- To ensure fairness, these Actively Engaged discounts will be applied to the Actively Engaged PPS targets
- PPSs are required to report non–duplicated numbers in IPP as communicated by the IA
Discussion Points
- Why is it necessary to discount "by PPS, by project" instead of "by county"?
- PPSs are not implementing their projects by county
- Applying a separate discount percentage by county is operationally unfeasible
- This approach was discussed and agreed upon with the stakeholder community
- In instances where a PPS is the only PPS to pursue a project in a given county, a 0% discount is factored into the final discount, as opposed to being removed from the final discount calculation entirely
Four Factors in Determining a PPS´ Discount Percentage
- 4 factors that will be used to determine the final discount percentage a PPS receives by project:
- The Percentage of Overlap Factor
- Discount Factors:
- Project 2.a.i Factor
- Sole County Factor
- Lack of Project Overlap Factor
Percentage of Overlap Factor
- The count of DSRIP Medicaid members with an interaction with providers in multiple PPS networks was determined ("Overlap"), by PPS by county
- Using the "Overlap" count by PPS by county, an "Overlap Percentage" was calculated
- The "Overlap Percentage" is the first component in determining a PPS´ actively engaged discount
By PPS By County [A] Overlap Count of Members with Provider Interactions that cross multiple PPSs [B] Non–Overlap Count of Members with Provider Interactions confined to a Single PPS [A] / [A + B] Overlap Percentage Forestland PPS Albany 100,000 300,000 25% Forestland PPS Saratoga 2,000 8,000 20% Forestland PPS Schenectady 30,000 60,000 33.3%
Discount Factors
- Once an "Overlap Percentage" is calculated, a set of discount factors are applied at the project level as follows:
| By PPS | By County | By Project | Overlap Percentage (Derived from County) |
|---|---|---|---|
| Forestland PPS | Albany | 2.a.i | 25% |
| Forestland PPS | Albany | 3.a.ii | 25% |
| Forestland PPS | Albany | 3.d.iii | 25% |
| Forestland PPS | Saratoga | 2.a.i | 20% |
| Forestland PPS | Saratoga | 3.a.ii | 20% |
| Forestland PPS | Saratoga | 3.d.iii | 20% |
| Forestland PPS | Schenectady | 2.a.i | 33.3% |
| Forestland PPS | Schenectady | 3.a.ii | 33.3% |
| Forestland PPS | Schenectady | 3.d.iii | 33.3% |
Discount Factor 1: 2.a.i
- Once an "Overlap Percentage" is calculated, a set of discount factors are applied at the project level as follows:
- 2.a.i–Because project 2.a.i´s objectives are to create an Integrated Delivery System, no discount will be applied to this project
| By PPS | By County | By Project | Overlap Percentage |
|---|---|---|---|
| Forestland PPS | Albany | 3.a.ii | 25% |
| Forestland PPS | Albany | 3.d.iii | 25% |
| Forestland PPS | Saratoga | 3.a.ii | 20% |
| Forestland PPS | Saratoga | 3.d.iii | 20% |
| Forestland PPS | Schenectady | 3.a.ii | 33.3% |
| Forestland PPS | Schenectady | 3.d.iii | 33.3% |
Discount Factor 2: Sole County
- Once an "Overlap Percentage" is calculated, a set of discount factors are applied at the project level as follows:
- Sole County Factor–If a PPS is the only PPS active in a county, then the "Overlap Percentage" for that county does not factor into the final discount calculation
| By PPS | By County | By Project | Overlap Percentage |
|---|---|---|---|
| Forestland PPS | Albany | 3.a.ii | 25% |
| Forestland PPS | Albany | 3.d.iii | 25% |
| Saratoga | |||
| Saratoga | |||
| Forestland PPS | Schenectady | 3.a.ii | 33.3% |
| Forestland PPS | Schenectady | 3.d.iii | 33.3% |
Assume that Forestland is the only
PPS active in Saratoga County
Discount Factor 3: Lack of Project Overlap
- Once an "Overlap Percentage" is calculated, a set of discount factors are applied at the project level as follows:
- Lack of Project Overlap Factor–If a PPS is the only PPS pursuing a project in a given county, then the "Overlap Percentage" is set to 0% (but it is still factored into the discount)
| By PPS | By County | By Project | Overlap Percentage |
|---|---|---|---|
| Forestland PPS | Albany | 3.a.ii | 25% |
| Forestland PPS | Albany | 3.d.iii | 25% |
| Forestland PPS | Schenectady | 3.a.ii | 33.3% |
| Forestland PPS | Schenectady | 3.d.iii | 0% |
Assume that Forestland is the only
PPS pursuing 3.d.iii in Schenectady County
Weighted Average–Discount by Project
- After the application of the business rules, the "Overlap Percentage" by county by project is weighted by the utilizing members attributed to the PPS in a given county
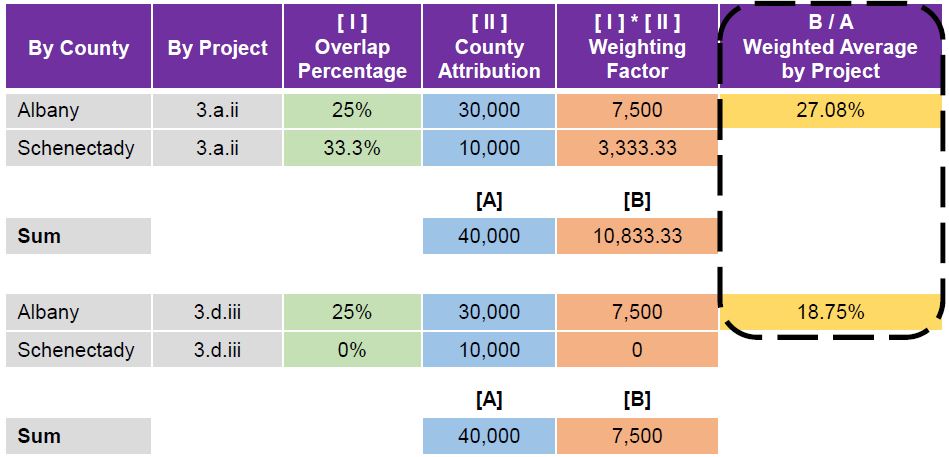
Final Actively Engaged Discounts
- This weighted average result is rounded UP to the nearest 5% integer
- This percentage is the discount factor applied to the actively engaged targets by PPS, by project
- Actively engaged targets will be communicated to the PPS next week, and will have the discount percentages applied, where applicable
| By PPS | By Project | As a Percentage |
↓ Rounded Up to the Nearest 5% |
|---|---|---|---|
| Forestland PPS | 3.a.ii | 27.08% | 30% |
| Forestland PPS | 3.d.ii | 18.75% | 20% |
Application of Actively Engaged Discounts
- The Final Actively Engaged Discounts have been applied, where applicable, to the quarterly Actively Engaged commitment targets from the DY1, Q1 Quarterly Report to determine the new Actively Engaged commitment targets.
- PPS will need to engage of minimum of 80% of the new Actively Engaged commitment target to earn the Achievement Value for respective quarter.
| PPS | Project | Original Actively Engaged Commitment DY1, Q4 |
Actively Engaged Discount Factor |
New Actively Engaged Commitment DY1, Q4 |
Minimum Actively Engaged to earn AV |
|---|---|---|---|---|---|
| Forestland PPS | 3.a.ii | 8,500 | 30% | 5,950 | 4,760 |
| Forestland PPS | 3.d.ii | 2,100 | 20% | 1,680 | 1,344 |
Interpreting the Comprehensive Provider Attribution (CPA) Report
Purpose
- The purpose of the Comprehensive Provider Attribution (CPA) report is to:
- Provide the PPS with the member level detail of their attributed cohort
- Catalog all Medicaid providers who performed a service on a PPS´ attributed member
- Display the number of visits by provider for each attributed PPS member
Providers in the CPA
- The CPA:
- Includes only a PPS´ attributed members
- Does not include members attributed to another PPS
- Includes member interactions with all Medicaid providers, not just member interactions with the PPS´ in–network providers
- Each record within the CPA will include a field denoting the provider that was responsible for an attribution, as well as a field denoting a servicing provider that did not result in an attribution
- A flag will be included for each provider to identify whether the provider is:
- In the PPS network being reported on
- In a PPS network not being reported on
- Not in any PPS network
- In PPS and in Other PPS
CPA Service Types
- For each member, the method of attribution that will be disclosed align with the DSRIP Attribution Loyalty Assignment (i.e. DSRIP Attribution Swimlane)
| Attributed Provider Service Type |
Non–Attributed Provider Service Type |
CPA Service Type Full Name |
|---|---|---|
| DD–R | DDL1 | Developmental Disabilities–Residential (Waiver and IID) |
| DD–DVS | DDL2 | Developmental Disabilities–Day/Vocational Services |
| DD–CM | DDL3 | Developmental Disabilities–Care Management |
| DD–A16 | DDL4 | Developmental Disabilities–Article 16 Clinic |
| DD–OWS | DDL5 | Developmental Disabilities–Other OPWDD Waiver Services |
| LTC–NH | LTCL1 | Long Term Care–Nursing Home |
| BH–HH | BHL1 | Behavioral Health–Health Home TC, or ACT or HCBS Waiver (kids) |
| BH–IRC | BHL2 | Behavioral Health–Intermediate or Intensive Residential Care (RTF, RRSY, Rehab Services to CR Residents, etc.) |
CPA Service Types
| Designation for provider that resulted in attribution |
Designation for provider that a member saw but did not result in attribution |
DSRIP Attribution Loyalty Assignment (i.e. DSRIP Attribution Swimlane) |
|---|---|---|
| Attributed Provider Service Type |
Non–Attributed Provider Service Type |
CPA Service Type Full Name |
| DD–R | DDL1 | Developmental Disabilities–Residential (Waiver and IID) |
| DD–DVS | DDL2 | Developmental Disabilities–Day/Vocational Services |
| DD–CM | DDL3 | Developmental Disabilities–Care Management |
| DD–A16 | DDL4 | Developmental Disabilities–Article 16 Clinic |
| DD–OWS | DDL5 | Developmental Disabilities–Other OPWDD Waiver Services |
| LTC–NH | LTCL1 | Long Term Care–Nursing Home |
| BH–HH | BHL1 | Behavioral Health–Health Home TC, or ACT or HCBS Waiver (kids) |
| BH–IRC | BHL2 | Behavioral Health–Intermediate or Intensive Residential Care (RTF, |
| BH–OC | BHL3 | Behavioral Health–OMH/OASAS Outpatient Clinic, CDT, PROS, Day Treatment, MMTP, Outpatient Rehab |
| BH–FMD | BHL4 | Behavioral Health–Freestanding MD psychiatrist, psychologist treating BH |
| BH–SM | BHL5 | Behavioral Health–Specialty Medical or Inpatient/ED for BH |
| AO–HH | OTHL1 | All Other–Health Home (Members meeting HH standard and Utilizing HH) |
| AO–PCP | OTHL2 | All Other–Primary Care Provider |
| AO–OPCP | OTHL3 | All Other–Other Primary Care Provider or Outpatient Clinic |
| AO–ED | OTHL4 | All Other–Emergency Department |
| AO–IP | OTHL5 | All Other–Inpatient |
| OTH CAT | (blank) | Other Category (not in any of the 16 Service Types defined above) |
Hypothetical Walk–Through
The following slides will walk users through a hypothetical example, using John Doe, a Medicaid Member in the State of New York. When reading through the example, please refer to the table at the bottom of each slide, which describes and defines the columns used throughout the CPA report.
- Medicaid member John Doe [MBR_ID = XYZ123] is attributed to the Forestland PPS [PPS_ID = FL2] and lives in Saratoga County [MBR_RES_COUNTY_CD = 41].
| Report Column Name | Description | Example |
|---|---|---|
| MBR_ID | The Member attributed to the PPS listed in column 'PPS ID' | XYZ123 |
| PPS_ID | The Performing Provider System (PPS) ID | Forestland PPS (FL2) |
| MBR_RES_COUNTY_CD | The member´s residence county code | 41 |
Hypothetical Walk–Through
(DSRIP Attributed Provider)
- John Doe is attributed to a DSRIP provider based on his claims volume [MBR_CATEGORY = Attributed Through Total Claims]. The attribution by provider service type is left blank in the CPA since the attribution resulted from total claims versus a specific qualifying service type [ATTR_PROV_SRV_TYPE = blank].
- The provider that led to John´s attribution–Maple Leaf [ATTR_PROV = 1930163744–Maple Leaf Recovery Inc.]–will appear on every record where John exists in the CPA.
| Report Column Name | Description | Example |
|---|---|---|
| MBR_CATEGORY | The Member´s attribution category. It will either contain one of the 16 CPA Service Types or one of the following reasons: – ´Attributed Through Total Claims´ – ´PCP Attributed´ | Attributed Through Total Claims |
| ATTR_PROV | The ´Attributed by´ provider´s NPI or MMIS Provider ID + Provider Name. When the Attr_Prov_Ind = ´Y´ in the source, this is the Attributed by provider for the member | 1930163744–Maple Leaf Recovery Inc. |
| ATTR_PROV_SRV_TYPE | The Attributed by provider Service Type | blank |
Hypothetical Walk–Through
(Non–Attributed Provider)
- John Doe also has an interaction with an Inpatient provider that belongs to one of the DSRIP Attribution Loyalty Assignments [Diag_Srv_Catg_CD = AO–IP].
- The Inpatient provider that John interacted with–[Prov_id = 1730686743] Dr. Sheryl Silverstein [Prov Name = Dr. Sheryl Silverstein]–did not lead to an attribution.
- Both the provider that led to attribution (Maple Leaf), and this specific provider (Dr. Sheryl Silverstein) will have relevant information listed on the same CPA record.
| Report Column Name | Description | Example |
|---|---|---|
| Prov id | CPA Service Type Provider ID related to the member within the PPS. Can either be an Entity ID or NPI. | 1730686743 |
| Prov Name | Service Type Provider Name related to the member within the PPS. Can either be an Entity ID or NPI. | Dr. Sheryl Silverstein |
| Diag_Srv_Catg_Cd | CPA Service Type. When this column is blank, this will be ´OTH CAT´. | AO–IP |
- Dr. Sheryl Silverstein processes 4 claims related to John Doe´s visits [Tot_Claim_Cnt = 4]. This is the provider to which John Doe has interacted with the second most [Prov_Seq = 2].
- Dr. Sheryl Silverstein is in the Forestland PPS and the Riverside PPS [Netwk_Ind = In PPS and Other PPS] networks.
| Report Column Name | Description | Example |
|---|---|---|
| Tot_Claim_Cnt | The total claims/encounters related to the Service Type Provider for the member within the PPS | 4 |
| Prov_Seq | The provider sequence number within the CPA Service Type. The providers are ranked by number of claims. Sequence 1 is ranked the highest | 2 |
| Netwk_Ind | Identifies whether the provider is:
|
In PPS and Other PPS |
Hypothetical Walk–Through
(Health Home Enrollment)
- John Doe does not have an open Health Home enrollment record [HH_IND = N]. For illustration purposes, if John Doe did have an open Health Home enrollment record, then [HH_IND = Y].
| Report Column Name | Description | Example |
|---|---|---|
| HH_IND | If member has an open Health Home enrollment record then this will be set to ´Y´. Otherwise, the indicator will be set to ´N´. | N |
Hypothetical Walk–Through
(Managed Care and PCP Assignment)
- John is enrolled with a Managed Care Organization [MCO = 01183019] called Spruce Health First [MCO_NAME = Spruce Health First].
- His MCO has assigned him a primary care provider [PCP_NPI = 1380008249], of which he regularly uses–Dr. Brown [PCP_NAME = Dr. Brown and Associates].
| Report Column Name | Description | Example |
|---|---|---|
| MCO | The provider ID of the member´s managed care organization (MCO) | 01183019 |
| MCO_NAME | The name of the member´s managed care organization | Spruce Health First |
| PCP_NPI | The NPI of the member´s MCO assigned primary care provider | 1380008249 |
| PCP_NAME | The name of the member´s MCO assigned primary care provider | Dr. Brown and Associates |
Hypothetical Walk–Through
(Summary)
| Report Column Name | Example Used |
|---|---|
| MBR_ID | XYZ123 |
| PPS_ID | Forestland PPS (FL2) |
| MBR_RES_COUNTY_CD | 41 |
| MBR_CATEGORY | Attributed Through Total Claims |
| ATTR_PROV | 1930163744–Maple Leaf Recovery Inc. |
| ATTR_PROV_SRV_TYPE | blank |
| Prov_id | 1730686743 |
| Prov Name | Dr. Sheryl Silverstein |
| Diag_Srv_Catg_Cd | AO–IP |
| Tot_Claim_Cnt | 4 |
| Prov_Seq | 2 |
| Netwk_Ind | In PPS and Other PPS |
| HH_IND | N |
| MCO | 01183019 |
| MCO_NAME | Spruce Health First |
| PCP_NPI | 1380008249 |
| PCP_NAME | Dr. Brown and Associates |
CPA Release Information
- The CPA reports will be sent to the PPS through the CMA Secure File Transfer Protocol (SFTP), where they will remain on–site at the location approved through the DEAA Agreement
- Because the CPA contains Member–Level data, the report can only be released to PPS currently cleared for data receipt, and can only be accessed by PPS users that had a User Identity Attestation
- PPS should hold the report centrally and redact once the opt–out process is complete
| Cleared for Data Receipt | |||
|---|---|---|---|
| Albany Medical Center | Finger Lakes | Alliance | CNYC C |
| Nassau Queens | Stony Brook | Bassett | Adirondack Health Institute |
| Montefiore | Refuah | Advocate Community Providers | Bronx Lebanon |
| Westchester Medical Center | NYU Lutheran | Maimonides | St. Barnabas Health |
| Mt. Sinai | NY Presbyterian–Queens | NY Presbyterian | Care Compass |
| Staten Island | Millennium Collaborative Care | Samaritan | Sisters of Charity |
| NYC Health & Hospitals Corp | |||
Future Attribution Reports
Overlap Report
- Purpose: The Overlap Report will show the count and percentage of overlapping members. These counts and percentages will be shown by provider, by PPS, by region.
- Release Date: ASAP
| Attribution Count | % of Total | Attribution Count | % of Total | Attribution Count | % of Total | Provider Total | |
|---|---|---|---|---|---|---|---|
| PPS 1 | PPS 2 | PPS 3 … | |||||
| Provider 1 | 400 | 14% | 2,000 | 69% | 500 | 17% | 2,900 |
| Provider 2 | 680 | 26% | 750 | 29% | 1,200 | 46% | 2,630 |
| Provider 3 | 45 | 26% | 62 | 36% | 66 | 38% | 173 |
| Provider 4 | 502 | 64% | 49 | 6% | 238 | 30% | 789 |
| PPS Total | 1,627 | 2,861 | 2,400 | ||||
The Individual Provider Attribution (IPA) Report
- Purpose: The IPA will show each PPS how many attributed member counts their providers had at the individual provider level. Results have been de–duplicated
- Release Date: The IPA report is scheduled for release the week of March 21st, 2016.
- This report will contain no PHI and be available to all PPSs
Questions?
DSRIP Email:
dsrip@health.ny.gov

Follow Us