Board for Professional Medical Conduct 2002-2004 Annual Report
- Board for Professional Medical Conduct 2002-2004 Annual Report is also available in Adobe Portable Document format. (PDF, 233KB, 15pg.)
New York State Department of Health
433 River Street, Suite 1000
Troy, NY 12180-2299
- Main Number: 518-402-0836
- Complaints/Inquiries: 1-800-663-6114
- E-mail Inquiries: opmc@health.state.ny.us
- Physician Information: www.nydoctorprofile.com or www.health.state.ny.us
George E. Pataki, Governor
Antonia C. Novello, M.D., M.P.H., Dr. P.H., Commissioner of Health
Dennis J. Graziano, Director
Office of Professional Medical Conduct
Kendrick A. Sears, M.D., Chair Michael A. Gonzalez, R.P.A.-C, Vice Chair
Board for Professional Medical Conduct Board for Professional Medical Conduct
Ansel R. Marks, M.D., J.D., Executive Secretary
General Program Information
Board for Professional Medical Conduct
The Board for Professional Medical Conduct (board) was created by the New York State Legislature in 1976 and serves as a key resource in the state's disciplinary oversight of physicians and physician assistants.
Public Health Law, Section 230(14) states:
The board shall prepare an annual report for the legislature, the governor and other executive offices, the medical profession, medical professional societies, consumer agencies and other interested persons.
Prior to 1976, the New York State Education Department was responsible for the licensing and disciplining of physicians and physician assistants. In 1976, the state Legislature split the licensing and disciplinary processes between the Departments of Education and Health. The board became responsible for investigating complaints, conducting hearings and recommending disciplinary actions to the State Education Department. The State Education Department and the Board of Regents, the department's governing body, were responsible for determining final actions in all physician discipline cases.
In 1991, the physician disciplinary process was again modified by the State Legislature. The Board of Regents and State Education Department were entirely removed from the physician discipline process. The State Education Department retained licensing authority, while the Department of Health assumed disciplinary authority, including the revocation of licenses, for physicians, physician assistants and specialist assistants. The Board for Professional Medical Conduct was granted sole responsibility for determining final administrative actions in all physician, physician assistant and specialist assistant discipline cases. All other health care professionals (e.g., nurses, dentists, podiatrists, etc.) are licensed and disciplined by the State Education Department.
The board serves as a key component in the state's disciplinary process. The board's mission is to protect the public from medical negligence, incompetence and illegal or unethical practice by physicians, physician assistants and specialist assistants. Physician members are appointed by the Commissioner of Health with recommendations for membership received largely from medical and professional societies. The Commissioner of Health, with approval of the Governor, appoints lay members of the board. By law, the Board of Regents may appoint 20 percent of the board's membership. The board's membership at the end of 2004 was comprised of 114 physicians (representing 24 different medical specialties) and 54 lay members, of whom 5 are physician assistants.
In disciplinary matters, board members serve on committees consisting of two physicians and one non-physician, who are appointed by the board chair. Disciplinary committees include investigation, hearing and license restoration. The Administrative Review Board (ARB) is a standing committee consisting of three physicians and two lay members. Board members also serve on a variety of committees that address procedural and emerging policy issues.
The roles of the board and the Office of Professional Medical Conduct (OPMC) are delineated in Public Health Law Section 230. The definitions of misconduct are found in Sections 6530 and 6531 of the Education Law.
Office of Professional Medical Conduct
OPMC provides staff to carry out the objectives of the board. OPMC's mission is to protect the public through the investigation of professional misconduct issues involving physicians. (In this report, when using the term physician, it refers to licensed MDs, DOs, and licensed, certified physician assistants and specialist assistants.) Through its investigative and monitoring activities, OPMC strives to deter medical misconduct and promote and preserve the highest standards of medical practice.
The office:
- Investigates all complaints and, with assistance of counsel, prosecutes physicians formally charged with misconduct.
- Monitors physicians whose licenses have been restored following a temporary surrender due to incapacity by drugs, alcohol or mental impairment.
- Oversees the contract with the Medical Society of the State of New York's Committee for Physicians' Health (CPH) – a non-disciplinary program to identify, refer to treatment and monitor impaired physicians.
- Monitors physicians placed on probation.
- Supports the activities of the board, including managing the appointment process, training, assisting with committee work and policy development, recruitment of medical experts, and coordinating the canvass procedures for approximately 150 hearing panels that are convened annually.
Overview of New York's Medical Conduct Process
OPMC is required by law to investigate every complaint it receives. Many complaints involve issues over which OPMC has no jurisdiction or authority, such as billing disputes or physician rudeness. In these instances, a physician is not aware of the complaint because they are closed administratively. In other cases, a complaint is investigated but insufficient evidence is found to support charges of misconduct, and the investigation is concluded.
When someone does file a complaint with OPMC that appears to involve possible misconduct, the physician will be notified either by letter or through a phone call. Generally, unless specifically stated otherwise, a letter requesting patient records is an indicator that a complaint has been filed against a physician and an investigation is underway. An investigator may call and say there is a complaint and ask for records or to discuss the matter.
State Public Health Law requires OPMC to keep confidential the names of any individuals who file complaints. The source of a complaint may not necessarily be the patient whose medical records are requested, but rather a friend, relative or health care worker. Sometimes patient medical records are requested because a health facility has reported to OPMC, as required by law, that it has taken disciplinary action against a physician.
While the law protects the identity of the complainant, it also preserves a physician's right to be heard. State Public Health Law requires that a physician be given the opportunity to be interviewed by OPMC staff to provide an explanation of the issues under investigation if the matter is going to be referred to the board. This interview may be conducted in person or over the telephone, and the physician may have an attorney present.
In many cases, even if the matter does not result in a referral to the board, the physician is contacted to respond to the issues in the complaint. Cases are not referred to the board when there is insufficient evidence to proceed or the issues are out of its jurisdiction. Physicians contacted in such cases are advised by letter that the matter is closed.
When an investigation finds evidence that appears to indicate that misconduct has occurred, the evidence is presented to an investigation committee of the board for review. If a majority of the investigation committee concurs with the Director of OPMC that sufficient evidence exists to support misconduct and after consultation with the Executive Secretary to the Board, the Director shall direct counsel to prepare charges.
The committee may recommend to the Commissioner of Health that a physician's practice be summarily suspended because he or she poses an imminent danger to the public health. If the Director of OPMC, after obtaining the concurrence of a majority of a committee on professional conduct, and after consultation with the Executive Secretary, determines that there is substantial evidence of professional misconduct of a minor or technical nature or of substandard medical practice which does not constitute professional misconduct, the Director may issue an administrative warning and/or provide for consultation with a panel of one or more experts, chosen by the Director. Administrative warnings and consultations are confidential.
If the case proceeds to a hearing or the Commissioner of Health orders a summary suspension, another three-member panel, including two physicians and a lay member, is drawn from the board. A hearing is much like a trial, although in this case the board panel serves as the jury and may also ask questions. An administrative law judge is present to assist the panel on legal issues. The state's case is presented by a staff attorney and physicians generally also choose to be represented by counsel. At the hearing, evidence is presented and testimony may be given by witnesses for both sides.
Public Health Law requires that hearings start within 60 days of the service of charges or, in cases of summary suspension, the hearing must commence within 10 days of the service of charges. The last hearing day must be held within 120 days of the first hearing day. The hearing panel's decision must be issued within 60 days of the last hearing day. Changes in these time frames can be made by agreement of both sides.
A hearing panel may decide to dismiss some or all of the charges against a physician. If the panel sustains charges, penalties can range from a censure and reprimand to revocation. The panel may also suspend or annul a physician's license, limit his or her practice, require supervision or monitoring of a practice, order retraining, levy a fine or require public service. Revocations, actual suspensions and license annulments are immediately made public and penalties go into effect at once.
Other penalties are not made public until the period for requesting an appeal has passed and, if there is an appeal, disciplinary action is stayed until there is a resolution. Either side may appeal the decision of a hearing panel to the ARB.
Notices of appeal to the ARB must be filed within 14 days of the service of a hearing committee decision. Both parties have 30 days from the service of the notice of appeal to file briefs and another 7 days to file a response to the briefs. There are no appearances or testimony in the appeals process. During an appeal, revocations, actual suspensions and annulments are not stayed. However, other penalties are stayed until the ARB acts.
The ARB reviews whether or not the determination and penalty of the hearing committee are consistent with the hearing panel's findings and whether the penalty is appropriate. The ARB must issue a written determination within 45 days after the submission of briefs.
Board Highlights
Special Board Committees
The Joint Committee of the Committee for Physicians' Health (CPH) and the Board for Professional Medical Conduct (BPMC) is charged to develop recommendations that will enhance the continued efforts of New York State's impaired physician programs to both protect the public and assist physicians in need. Two subcommittees were appointed and charged with reviewing two specific issues (boundary issues and the restoration process) and making recommendations for the committee's consideration. Each subcommittee consists of four Joint CPH-BPMC Committee members and one staff person from each program.
Physician/Patient Boundary Issues
The Subcommittee on Boundary Issues addressed concerns that physicians may not be fully aware of the issues and consequences surrounding boundary violations. The subcommittee focused on developing educational materials that would address several types of boundary issues (including financial, social and sexual) for physicians. Working with the authors' permission, the subcommittee modified an article entitled "Professional Boundaries in the Physician-Patient Relationship" by Glenn Gabbard, M.D. and Carol Nadelson, M.D. The Department posted the revised article on its web site in 2004 and the Medical Society of the State of New York published the article in its monthly news journal. Copies were also shared with each member of the Board for Professional Medical Conduct.
Enhancing the Restoration Process
Each year physicians petition the board for approval to return to the active practice of medicine following treatment for their impairment. The restoration process involves an informal proceeding during which a committee of the Board reviews records and hears testimony regarding the fitness of the physician to practice safely and competently. The Subcommittee on Enhancing the Physician's License Restoration Process (subcommittee) developed written procedures, which were implemented by the board in 2004, to help guide physicians through the restoration process. The revised procedures were designed to streamline the process affording physicians, who demonstrate recovery and competence, the opportunity to return to the practice of medicine in a more timely manner.
The subcommittee continues to explore relevant issues associated with license restoration, including identification of:
- Additional behavioral health specialists to conduct clinical assessments
- "Milestones" of recovery
- Hospital reporting issues
Biennial Meeting
The 2004 Biennial Meeting of the Board for Professional Medical Conduct was held in Albany on November 20-21, 2004. One hundred and sixty nine members and staff, representing approximately 75% of the board, attended the weekend session. The Biennial Meeting is part of the board's ongoing efforts to provide training on contemporary issues pertinent to the practice of medicine and the disciplinary system.
The primary focus of the training workshops centered on the development of appropriate penalties as contained in Public Health Law, Section 230-A and included a comprehensive review of OPMC's physician monitoring programs.
Small groups were convened to study redacted disciplinary hearing cases and were charged with the responsibility of focusing on the development of appropriate penalties. The group's decision regarding appropriate penalties was then compared to the redacted copy of the decisions rendered by the disciplinary hearing committee and the Administrative Review Board. Throughout the process, facilitated discussions were convened with the small groups and the entire board. Electronic voting machines enhanced this process by providing for an immediate collation of the group's determinations and recommendations.
Federation of State Medical Boards
The Federation of State Medical Boards (FSMB) is a national not-for-profit organization representing 70 medical boards within the United States and its territories. As the representative body and forum for physician licensing and disciplinary boards, FSMB occupies a unique position of responsibility.
FSMB continues to view New York as a leader among state medical boards. At its 2004 annual meeting, FSMB re-elected Board members Fr. Daniel W. Morrissey to another term on its Board of Directors and Kendrick A. Sears, M.D. to the Nominating Committee. Calvin J. Simons, M.D. was appointed to the Bylaws Committee and the Director of OPMC was appointed to a three-year term on its Advisory Council of Board Executives. Other board members serve on various committees of FSMB or have been featured speakers at the Federation's Annual Meetings.
Program Highlights
- During the last five years, the average number of disciplinary actions taken per year is 333, a 34 percent increase over the average of 248 taken per year during 1992 -1996.
- During the last nine years, the number of complaints received has increased an average of 4 percent per year. In 2004, there was a 34 percent increase in complaints received (6,925) compared to the number of complaints received (5,151) in 1996.
- In 2004, 77 percent of the complaints received during the year were resolved as opposed to only 59 percent of the complaints having been resolved in 1996.
- The average length of time for case prosecution has decreased from 6 months in 1996 to under 5 months in 2004.
- The average length of time for complaint investigation has decreased from 7 months in 1996 to under 4 months in 2004.
- OPMC continued to aggressively prosecute physicians who violate their terms of probation by referring 24 physicians for prosecution and taking 15 disciplinary actions, 12 of which involved loss of license.
- A 2004 report from the Federation of State Medical Boards states that in 2003, New York took more disciplinary actions that resulted in loss of license than any other large state.
- The Public Citizen Group ranked New York 14th in the nation in its 2004 analysis of state boards. In 1991, New York ranked 49th.
Legislative Activity (Proposed Amendments to Public Health Section 230)
In January 2002, representatives of the Department and OPMC testified before a joint committee of the New York State Assembly Health, Higher Education and Codes Committees regarding the physician discipline process in New York State. The purpose of the hearing was to examine whether important elements of due process are lacking and whether there are ways to expedite the process, to better protect the public and rights of the accused.
Following the hearing, legislation to amend the physician discipline process was introduced by the New York State Legislature in 2002, 2003 and 2004. Legislation passed both houses of the Legislature in 2004.
The proposed amendments to Public Health Law Section 230 provided for procedural and substantive changes to many areas of the process, including the definition of lay members of the Board, the physician interview process, investigation committee procedures and hearing and appeal processes. In addition, the bill included provisions for an evaluation program to determine a physician's competency to practice medicine and an informal settlement conference to resolve cases of medical misconduct.
Governor Pataki vetoed the legislation in 2004, citing concern that the bill could result in unnecessary and inappropriate delays in the process and impede the efforts of OPMC and the board to protect the public against the small minority of physicians who are guilty of misconduct. The Governor also noted his unwillingness to compromise the dramatic improvements that New York has achieved in this program area over the last ten years by approving a series of procedural and substantive changes that could make the process more cumbersome and complex.
Legislative Activity (Crime Reporting Responsibility)
In September 2003, Governor Pataki signed legislation requiring the board or OPMC to notify the appropriate district attorney when, based upon a reasonable belief, a criminal offense has been committed by a physician. As of the end of 2004, 11 referrals have been made.
Medical Quality Assurance Program
An integral component of OPMC's investigations is the clinical review conducted by outside medical experts and physician staff members particularly in those cases involving negligence, incompetence and impairment issues.
It was recognized that implementation of a formalized, statewide Medical Quality Assurance Program that codified what constituted an appropriate clinical review within the unique context of the medical conduct program would serve to reinforce the objectivity and integrity of the investigative process.
A statewide program for medical reviews was developed and implemented that established uniform standards and procedures and employs an ongoing review and monitoring process. Since the program's deployment, training needs and strategies for addressing these needs have been identified. Formal procedures for conducting progress reviews and providing feedback to Medical Coordinators and investigations management staff have been established.
Case Management Information System
A customized case management information and tracking system, to support OPMC investigative operations, was designed and successfully beta tested. Statewide implementation of the new system, which began in 2004, is expected to be completed by the end of 2005.
This case management tool significantly improves the efficiency and effectiveness of case investigations. It offers OPMC management and investigators "real time" and immediate access to all investigative materials that will be stored electronically in a centralized location. The system will also allow for a seamless integration of multiple data systems and enhanced search and retrieval capabilities.
Streamlining
OPMC receives nearly 7,000 complaints per year and is required, by law, to investigate every complaint it receives. All complaints receive a preliminary review to determine whether the allegations fall within the jurisdiction of the office. Once jurisdiction is established, an investigation is initiated.
In an effort to focus investigative resources and to quickly identify those cases which may represent significant potential for patient harm, an investigative streamlining strategy was implemented.
This approach allows supervisors and managers to focus investigative resources on those cases having strong potential for successful prosecution, based on the medical or legal merits of the case. Preliminary results indicate that cases with little potential for successful prosecution are identified quicker; investigators' caseloads have been reduced; and investigative resources are deployed more efficiently.
Two-Call Case Resolution
Many of the complaints received concerning physicians involve matters that are not serious in the sense of there being public harm, but are, nonetheless, very upsetting and serious to the complainant. A pilot program, "the two-call case resolution", was designed and tested in 2001 in an effort to identify and appropriately resolve non "serious" cases more quickly and efficiently to the satisfaction of both the complainant and the subject physician.
The two calls referred to are generally two telephone calls, one made to the complainant and one to the subject physician by a staff physician. Using this strategy, OPMC has been able to successfully close nearly 350 cases over a three-year period. This "two-call" approach significantly reduced or eliminated the need for resource depleting complainant and physician interviews and related investigative activity.
Internet Access to Physician Information
The New York Patient Health Information and Quality Improvement Act signed by Governor Pataki in 2000 provided for immediate access to physician information through the Internet.
Certain information is required to be available on all physicians who are registered in New York State and includes information such as: medical education, specialty board certifications, hospital privilege restrictions, malpractice history, criminal convictions and public disciplinary actions. Physicians may also provide extra information (optional information) including; practice locations, published research articles, professional and community service activities and health plan information. The physician profile information can be accessed through the Department's web site, www.health.state.ny.us or directly via www.nydoctorprofile.com.
Information regarding the Office and Board for Professional Medical Conduct can be accessed through the Department's web site, www.health.state.ny.us and click on "Physician Discipline." All disciplinary actions taken since 1990 are posted on OPMC's site, as well as information on how to file a complaint, brochures regarding medical misconduct, frequently asked questions, and relevant statutes.
Summary Statistics
| Year | |||||
|---|---|---|---|---|---|
| 2000 | 2001 | 2002 | 2003 | 2004 | |
| Complaints Received | 6106 | 6983 | 7295 | 6275 | 6925 |
| Investigations Completed | 5939 | 6854 | 7082 | 6882 | 6711 |
| Licensees Referred for Charges | 388 | 367 | 328 | 354 | 337 |
| Administrative Warnings/Consultations | 121 | 155 | 165 | 166 | 123 |
| Summary Suspensions* | 43 | 23 | 13 | 37 | 19 |
| Disciplinary Actions | Year | ||||
|---|---|---|---|---|---|
| 2000 | 2001 | 2002 | 2003 | 2004 | |
| Surrender | 97 | 97 | 86 | 61 | 85 |
| Revocation | 47 | 33 | 49 | 37 | 17 |
| Suspension | 105 | 101 | 99 | 116 | 116 |
| Censure and Reprimand/Probation | 34 | 32 | 33 | 51 | 55 |
| Censure and Reprimand/Other | 64 | 44 | 49 | 59 | 41 |
| Dismiss | 10 | 18 | 4 | 8 | 6 |
| Subtotal | <357 | <325 | <320 | <332 | <320 |
| Temporary/Permanent Surrenders | 25 | 18 | 8 | 13 | 23 |
| Monitoring Agreements | 29 | 25 | 21 | 27 | 44 |
| Total Actions | <411 | <368 | <349 | <372 | <387 |
* In 1996, Public Health Law 230 was amended to permit a summary suspension when a licensee has pleaded or been found guilty or convicted of committing an act constituting a felony under New York State Law or federal law, or the law of another jurisdiction which, if committed within this state, would have constituted a felony under New York state law, or when the duly authorized professional agency of another jurisdiction has made a finding substantially equivalent to a finding that the practice of medicine by the licensee in that jurisdiction constitutes an imminent danger to the health of its people.
Office of Professional Medical Conduct Source of Complaints 2004
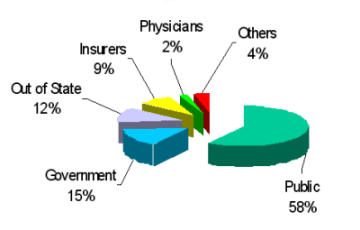
| Source of Complaint | Percentage |
|---|---|
| Government | 15% |
| Insurers | 9% |
| Other | 4% |
| Out of State | 12% |
| Physicians | 2% |
| Public | 58% |
Office of Professional Medical Conduct Disciplinary Actions:
Average Distribution by Type 2000-2004
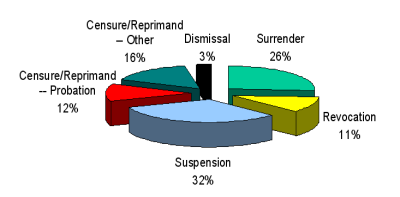
| Disciplinary Action | Percentage |
|---|---|
| Censure/Reprimand - Other | 16% |
| Censure/Reprimand - Probation | 12% |
| Dismissal | 3% |
| Revocation | 11% |
| Surrender | 26% |
| Suspension | 32% |
